- CSID Cares
- About CSID
- What Is Congenital Sucrase-Isomaltase Deficiency?
Congenital Sucrase-Isomaltase Deficiency (CSID) is a rare disorder that affects your ability to digest certain sugars due to absent or low levels of two digestive enzymes, sucrase and isomaltase. Sucrase and isomaltase are involved in the digestion of sugar and starches. Sucrase is the intestinal enzyme that aids in the breakdown of sucrose (table sugar) into glucose and fructose, which are used by the body as fuel. Isomaltase is one of several enzymes that help digest starches.1, 2
CSID is an inherited form of sucrose intolerance or sucrase deficiency. This disorder occurs with equal frequency in males and females.2

Sugar
Sucrose, a sugar found in fruits and known as table sugar, and isomaltose, a sugar found in grains, are called disaccharides because they are made of two simple sugars. Disaccharides are broken down into simple sugars during digestion by intestinal enzymes. Sucrose is broken down into glucose and fructose, and isomaltose is broken down into two glucose molecules. Individuals with CSID have an impaired ability to break down these disaccharides (sucrose and isomaltose) into simple sugars called monosaccharides (glucose and fructose) that the body uses as fuel. Typically, an individual with CSID has decreased, often absent, sucrase activity, decreased-to-normal isomaltase activity, and reduced maltase activity.3
Although simple sugars are the main carbohydrate absorbed in the digestive tract, monosaccharides (glucose, fructose, and galactose) are rarely found in human diets. Instead, disaccharides (for example, sucrose, lactose, and maltose) are more common in the human diet and must be broken down into monosaccharides by small intestinal enzymes before they can be absorbed into the bloodstream for use by the body. Without this breakdown, none of these disaccharides can be used for energy because they are too big to be absorbed by the intestine.
The small intestine is lined with finger-like projections called microvilli. The microvilli are known collectively as the brush border. The microvilli absorb nutrients from food as it passes through the small intestine.
The Digestive Tract

Enzymatic Reaction



Starch
Individuals with CSID have varying activity of the enzymes required for starch digestion, so they may also experience gastrointestinal symptoms after eating foods containing starch.
Carbohydrates
Carbohydrates are classified as either simple or complex. Classification depends on the chemical structure of the food, which affects how quickly the sugar is digested and absorbed. Simple carbohydrates have one sugar (monosaccharides) or two sugars (disaccharides). Complex carbohydrates have three or more sugars linked together (polysaccharides).
Many complex carbohydrates are starchy carbohydrates, which require ample time and adequate enzymatic activity in the digestive tract to be digested properly. Starch digestion depends on the combination of enzyme activities that occur at several sites in the gastrointestinal tract, from the salivary gland in the mouth, to the pancreas, to the brush border in the small intestine.
Monosaccharides
Simple sugars like glucose and fructose which are found in fruits and honey
Disaccharides
Two molecules of simple sugars such as sucrose, lactose, and maltose
Polysaccharides
Made up of a number of molecules of simple sugars, including starch, glycogen, and cellulose
Digestion of Starches

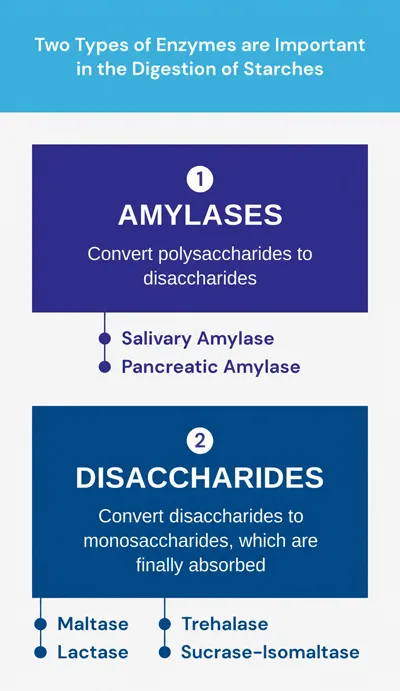
The digestion of starches begins in the mouth with an enzyme in saliva called salivary amylase, sometimes called ptyalin. Chewing grinds the food and breaks it apart, allowing salivary amylase to work more effectively. After swallowing, the starchy carbohydrates reach the stomach where gastric enzymes begin to break down food.
The stomach plays a major role in digestion by mechanically mixing and crushing the food and enzymatically by further breaking down food. The stomach also acts as a reservoir to facilitate the movement of smaller amounts of food into the small intestine at any given time. The stomach secretes a form of amylase called gastric amylase that further digests starches.
In the small intestine, starch is processed by an enzyme called pancreatic amylase and converted into maltose and isomaltose. Maltose and isomaltose must be broken down into simple sugars for the body to use as fuel. Individuals with CSID may have difficulty breaking down isomaltose, since they may lack the digestive enzymes of the brush border. Throughout the lining of the small intestine, there are normally numerous brush border enzymes (for example, sucrase, lactase, maltase) whose function is to further break down digested food into small, more absorbable particles.
Maltase-glucoamylase is a brush border enzyme that plays a role in the final steps of small intestinal digestion of starch to glucose. Isomaltase is an enzyme that breaks the bonds linking sugars that cannot be broken by amylase or maltase. Glucose is the end product of all starch digestion. After starch is broken down into glucose molecules, the small intestine transports the glucose molecules into the bloodstream, where they are distributed throughout the body to provide energy to virtually all cells, including the brain. If glucose is not immediately used, it may be stored in the liver or skeletal muscle for later use.
References
- Danialifar TF, Chumpitazi BP, Mehta DI, Di Lorenzo C. Genetic and acquired sucrase-isomaltase deficiency: A clinical review. J Pediatr Gastroenterol Nutr. 2024;78(4):774-82. doi:10.1002/jpn3.12151
- National Organization for Rare Disorders. Congenital sucrase-isomaltase deficiency. Last updated February 7, 2018. https://rarediseases.org/rare-diseases/disaccharide-intolerance-i/
- Naim HY, Heine M, Zimmer KP. Congenital sucrase-isomaltase deficiency: heterogeneity of inheritance, trafficking, and function of an intestinal enzyme complex. J Pediatr Gastroenterol Nutr. 2012;55(suppl 2):S13-20. doi:10.1097/01.mpg.0000421402.57633.4b